
Current state of burnout in medicine
First described by psychologist Herbert Freudenberger in 1974, burnout was initially observed among mental health workers (including himself) in a Mental Health Free Clinic setting.
In the 1980’s, Psychologist Chirstina Maslach further defined burnout, identifying three key components:
1.Emotional Exhaustion
2.Depersonalization
3.Decreased Sense of Accomplishment
Burnout is not currently classified as a mental disorder or a medical condition in the DSM-5
ICD-10 [Z70.3] and ICD-11 [QD85] have included burnout as an important occupational phenomenon, categorizing it under "factors influencing health status”, which includes reasons for which people contact health services but that are not classified as illnesses or health conditions.
So essentially, it is regarded as stress or dissatisfaction with one’s job. After mental health workers, it was first observed in other health care professionals.
Several studies show that burnout rate is consistently around 40-50% in health care professionals and other high demanding occupations. Other high-risk groups include parents, students and caregivers.
Burnout has traditionally been conceptualized through a psychological framework. However, a deeper exploration of its neurophysiological underpinnings suggests that it may be possible to identify, address, and even prevent burnout before its psychological manifestations become clinically apparent.
While we intend to formally test and validate our hypothesis regarding the neurological basis of burnout, there is an urgent need to share insights derived from an extensive review of the literature. Each week, we observe colleagues stepping away from clinical practice; whether by reducing their hours, transitioning to industry roles, or leaving the profession entirely; as a result of burnout. This trend exacerbates the existing shortage of physicians and advanced practice providers, further straining the healthcare system and perpetuating a self-reinforcing cycle.
Our goal is to increase awareness and knowledge about neurological changes in burnout, so individuals can take steps to address their burnout by lifestyle modifications.
Burnout Research
Selected Articles:
LaFaver K et al. Age and sex differences in burnout, career satisfaction, and well-being in US neurologists. Neurology. 2018 Nov 13;91(20):e1928-e1941.
This article was published in Neurology journal and describes factors associated with Burnout in US Neurologists.
Depersonalization score more than 10 or more is associated with burnout. It was mainly seen in younger neurologists and decreased with age. The next graph is for emotional exhaustion. For this, score more than 27 or more is associated with burnout, and a large population of neurologists reported that. Interestingly, it peaked around age 40. The next graph is for decreased personal accomplishment. For this measure, a score lower than 33 or lower is associated with burnout. A majority of the neurologist reported they still find their job valuable.
They put the data in multivariable logistic model and it came up with three groups: High risk, average risk and low risk for burnout (Figure 2). In all age groups, the risk of burnout was higher with age, peaked around age 40-50 and then decreased. There were no significant differences among males and females. For neurologists <65 years of age, the high risk group neurologists were at almost 90% risk of burnout. Medium risk group physicians were at between 60-70% while low risk physicians at 20-30% risk of burnout.
I took the liberty of putting the characteristics of each group in a table to better understand how do these groups differ (Figure 3). The High risk and low risk groups are aligned to what we would think. Some one who doesn’t have or autonomy, don’t find their work meaningful, has unreasonable amount of clerical tasks, doesn’t have effective support staff, work more hours, work on the weekends and nights while seeing the same amount of outpatients will be at much high risk of burnout compared to low risk group.
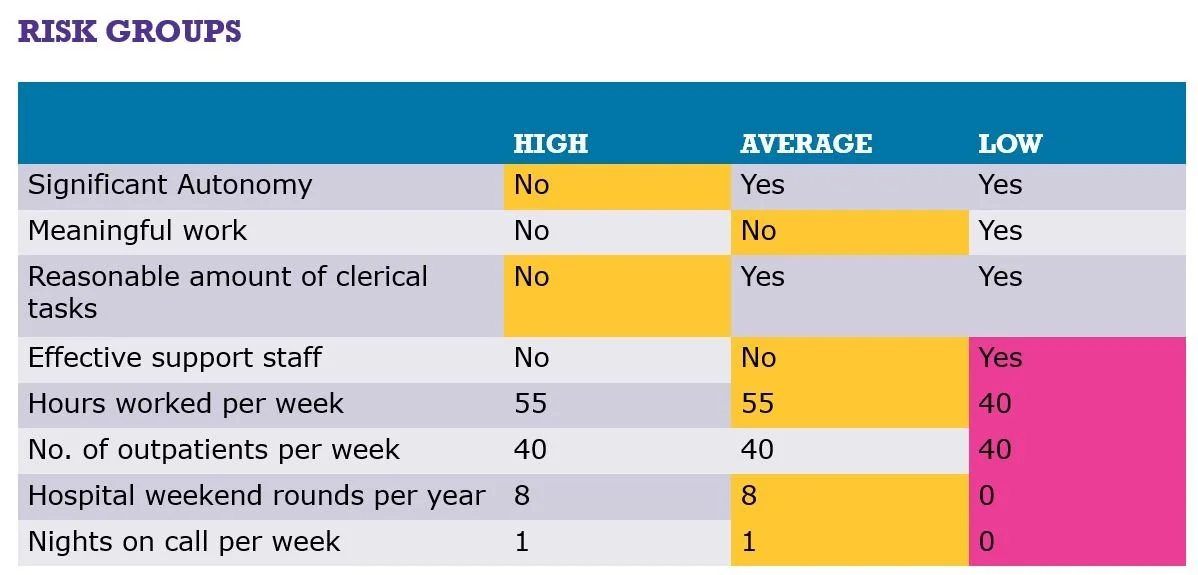
Figure 1: Characteristics of Risk group categories (based on Lafaver K. et al), Neurology. 2018 Nov 13;91(20):e1928-e1941
The high-risk group did not have significant autonomy, did not think their work was meaningful, did not have a reasonable amount of clerical tasks, did not have an effective support staff, worked 55 hours per week, saw 40 outpatients per week, had hospital rounds 8 weekends per year, and had 1 night on call per week. The average-risk group had significant autonomy, did not think their work was meaningful, had a reasonable amount of clerical tasks, did not have an effective support staff, worked 55 hours per week, saw 40 outpatients per week, had hospital rounds 8 weekends per year, and had 1 night on call per week. The low-risk group had significant autonomy, thought their work was meaningful, had a reasonable amount of clerical tasks, had an effective support staff, worked 40 hours per week, saw 40 outpatients per week, had hospital rounds 0 weekends per year, and had 0 nights on call per week.
Reflection Question for Readers: Which category do you fall in?
A bigger question: Is burnout really a tired brain, a stressed mind, or combination of both? We need to understand the neuroanatomy and neurophysiology of burnout to answer that question.
_________________________________________________________________________________
The role of Prefrontal Cortex in Burnout
In a prospective, randomized and cross-over study on 74 ICU nurses, the researchers measured cerebral oxygenation levels on night and day shift using a near-infrared spectroscopy system.
Results: The average regional saturation (rSO2) index in dorsolateral prefrontal cortex decreased significantly in the night shift. There was also decrease in the verbal fluency test and increase in anxiety score in night shift. Interestingly, getting 2 hours of sleep during the nightshift was significantly associated with better outcomes in these tests compared to 0 hours of sleep.
So, there are changes in the brain happening with lack of sleep and some getting some sleep during these stressful and high demand periods is helpful.
Reference:
Duran-Gomez, N., et al., Night Shift and Decreased Brain Activity of ICU Nurses: A Near-Infrared Spectroscopy Study. Int J Environ Res Public Health, 2021. 18(22)._________________________________________________________________________________
In another study, The burnout group at intake had reduced thickness in the right prefrontal cortex (PFC) and left superior temporal gyrus (STG), enlarged amygdala volumes, and reduced caudate volumes. All changes except caudate volumes were more pronounced in women. Thickness of the PFC also correlated with an impaired ability to down-modulate negative emotions. Do you find yourself snap especially at loved ones for little things when you are overworked?
Now surprisingly, Thinning of PFC and reduction of caudate volume normalized after 1-2 years of cognitive therapy. So some of the changes in burnout patients are reversible with therapy.
Reference:
Savic, I., A. Perski, and W. Osika, MRI Shows that Exhaustion Syndrome Due to Chronic Occupational Stress is Associated with Partially Reversible Cerebral Changes. Cereb Cortex, 2018. 28(3): p. 894-906._________________________________________________________________________________
In another study, near infrared spectroscopy showed reduced brain activity over fronto polar and dorsolateral prefrontal region in the patients with burnout during verbal fluency test.
Reference:
Chou et al. Perceived Occupational Stress is associated with Decreased Cortical Activity of the Prefrontal Cortex: A Multichannel Near-infrared Spectroscopy Study. Scientific reports, 12/2016, Volume 6, Issue 1So multiple studies show that prefrontal cortex, specifically dorsolateral PFC is involved in the patients reporting burnout.
Besides dorsolateral prefrontal cortex, there are several other areas of brain that show increased or decreased activity, volume and function per different neuroscientific studies. This suggests that there are neurological mechanisms (and not just psychological mechanisms) that lead to, or are results of burnout process.